INHERITING HUNTER'S SYNDROME and LIFE EXPECTANCY
Here is where genetics play a key role in determining whether or not a couple’s children will be affected by Hunter’s Syndrome. Hunter’s Syndrome is an inherited disease. It is carried in the X-linked recessive gene passed from the mother to her children. Naturally, if a woman finds out that she is a carrier of the disease, she will have some apprehension regarding giving birth to her own children. It is important to note that not every child the mother gives birth to will suffer from Hunter’s Syndrome.
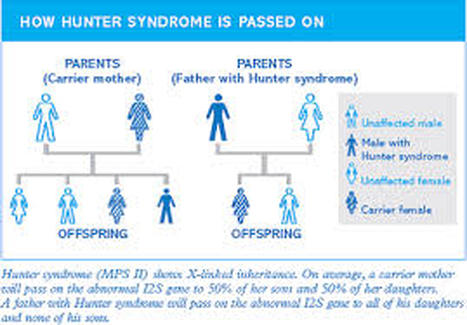
The gene that the child receives from its father will not play a role in the inheritance of Hunter’s Syndrome. Once the mother has been identified as a carrier and gives birth to a recessive gene, he will inherit Hunter’s Syndrome. Tests will have to be done and the family may have to wait to find out until later in the child’s life if he has Hunter’s Syndrome. It is possible for him to receive the dominant and unaffected X chromosome from his mother and not develop Hunter’s Syndrome.
If the mother is a carrier with an abnormal X chromosome and gives birth to a female, that child may potentially be a carrier of the disease but will most likely never show signs or symptoms of the disease. This is where the father’s chromosome plays a big part. The X chromosome that the female child receives from her father allows the child to be unaffected by the abnormal chromosome she receives from her mother. There is a one in four chance that a carrier mother will give birth to a child that will suffer from Hunter’s Syndrome (Wraith et al., 2008).
It is possible for the female child to receive both dominant X chromosomes from her parents and her children will not be at risk for carrying the disease. This is probably the best and most wished upon scenario for any family that is battling with Hunter’s Syndrome. If none of the mother’s children are carriers of the disease, then her grandchildren will have escaped all possibility of inheriting the disease.
The gene that the child receives from its father will not play a role in the inheritance of Hunter’s Syndrome. Once the mother has been identified as a carrier and gives birth to a recessive gene, he will inherit Hunter’s Syndrome. Tests will have to be done and the family may have to wait to find out until later in the child’s life if he has Hunter’s Syndrome. It is possible for him to receive the dominant and unaffected X chromosome from his mother and not develop Hunter’s Syndrome.
If the mother is a carrier with an abnormal X chromosome and gives birth to a female, that child may potentially be a carrier of the disease but will most likely never show signs or symptoms of the disease. This is where the father’s chromosome plays a big part. The X chromosome that the female child receives from her father allows the child to be unaffected by the abnormal chromosome she receives from her mother. There is a one in four chance that a carrier mother will give birth to a child that will suffer from Hunter’s Syndrome (Wraith et al., 2008).
It is possible for the female child to receive both dominant X chromosomes from her parents and her children will not be at risk for carrying the disease. This is probably the best and most wished upon scenario for any family that is battling with Hunter’s Syndrome. If none of the mother’s children are carriers of the disease, then her grandchildren will have escaped all possibility of inheriting the disease.
Due to the fact that there is a different rate of progression in the progressively debilitating disorder, there is a wide range of ages for life expectancy in individuals with Hunter’s Syndrome. As discussed earlier, the severe form presents itself earlier in the child’s life while the less severe presents later into the toddler stage of life.
If an individual suffers from the severe form, his life expectancy is between 10 and 20 years of life. They will steadily begin to lose the basic functional life skills that they have learned as they move closer to the end of their life (“Mucopolysaccharidosis type II,” 2014). Individuals with the less severe form of the disease will most likely live to reach adulthood and will make intellectual advances.
If an individual suffers from the severe form, his life expectancy is between 10 and 20 years of life. They will steadily begin to lose the basic functional life skills that they have learned as they move closer to the end of their life (“Mucopolysaccharidosis type II,” 2014). Individuals with the less severe form of the disease will most likely live to reach adulthood and will make intellectual advances.
